


 Sign Out
Sign Out

DUROGESIC doses should be individualized based upon the status of the patient and should be assessed at regular intervals after application. The patches are designed to deliver approximately 12, 25, 50, 75, and 100 mcg/h fentanyl to the systemic circulation, which represent about 0.3, 0.6, 1.2, 1.8, and 2.4 mg per day, respectively.
Initial dosage selection: The appropriate initiating dose of DUROGESIC should be based on the patient's current opioid use. It is recommended that DUROGESIC be used in patients who have demonstrated opioid tolerance. Other factors to be considered are the current general condition and medical status of the patient, including body size, age, and extent of debilitation as well as degree of opioid tolerance.
Adults: Opioid-tolerant patients: To convert opioid-tolerant patients from oral or parenteral opioids to DUROGESIC, refer to Equianalgesic potency conversion as follows. The dosage may subsequently be titrated upwards or downwards, if required, in increments of either 12 or 25 mcg/h to achieve the lowest appropriate dosage of DUROGESIC depending on response and supplementary analgesic requirements.
Opioid-naïve patients: Clinical experience with DUROGESIC is limited in opioid-naïve patients. In the circumstance in which therapy with DUROGESIC is considered appropriate in opioid-naïve patients, it is recommended that these patients be titrated with low doses of immediate release opioids (e.g., morphine, hydromorphone, oxycodone, tramadol, and codeine) to attain equianalgesic dosage relative to DUROGESIC with a release rate of 25 mcg/h. Patients can then be converted to DUROGESIC 25 mcg/h. The dosage may subsequently be titrated upwards or downwards, if required, in increments of either 12 or 25 mcg/h to achieve the lowest appropriate dose of DUROGESIC depending on response and supplementary analgesic requirements (see Equianalgesic potency conversion as follows). (See also Opioid naïve and non-opioid tolerant states under Precautions.)
Equianalgesic potency conversion: Calculate the previous 24-hour analgesic requirement.
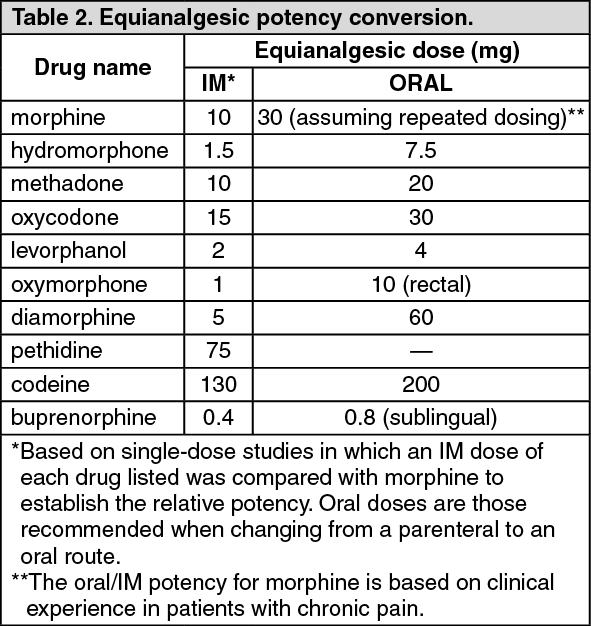
Convert this amount to the equianalgesic oral morphine dose using Table 2. All IM and oral doses in this chart are considered equivalent to 10 mg of IM morphine in analgesic effect.
To derive the DUROGESIC dosage corresponding to the calculated 24-hour, equianalgesic morphine dosage, use the dosage-conversion Table 3 [or the dosage-conversion Table 4] as follows: Table 3 is for adult patients who have a need for rotation of, or conversion from, another opioid regimen (conversion ratio of oral morphine to transdermal fentanyl approximately equal to 150:1).
[Table 4 is for adult patients who are on a stable, and well-tolerated, opioid regimen (conversion ratio of oral morphine to transdermal fentanyl approximately equal to 100:1).] (See Tables 2, 3 and 4.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image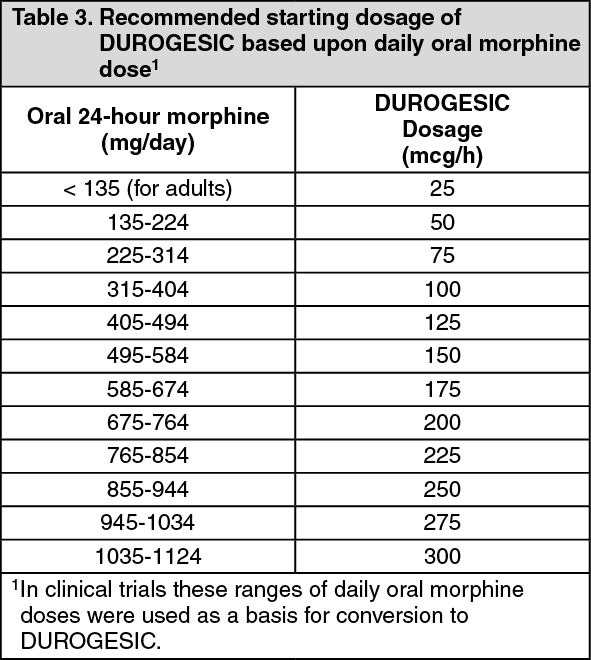 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageInitial evaluation of the maximum analgesic effect of DUROGESIC cannot be made before the patch is worn for 24 hours. This delay is due to the gradual increase in serum fentanyl concentration in the 24 hours following initial patch application.
Previous analgesic therapy should therefore be gradually phased out after the initial dose application until analgesic efficacy with DUROGESIC is attained.
Dose titration and maintenance therapy: A 12 mcg/h strength is available for dose titration. The DUROGESIC patch should be replaced every 72 hours. The dose should be titrated individually until a balance between analgesic efficacy and tolerability is attained. If analgesia is insufficient after the initial application, the dose may be increased after 3 days. Thereafter, dose adjustment can take place every 3 days. Early in therapy, some patients may not achieve adequate analgesia during the third day using this dosing interval and may require DUROGESIC patch to be applied at 48 hours rather than at 72 hours. Reducing the duration of system application by replacing the system before the 72 hours may result in increased serum concentrations of fentanyl (see Pharmacology: Pharmacokinetics under Actions).
Dosage titration should normally be performed in 12 mcg/h or 25 mcg/h increments, although the supplementary analgesic requirements (oral morphine 45/90 mg/day≈DUROGESIC 12/25 mcg/h) and pain status of the patient should be taken into account. More than one DUROGESIC patch may be used for doses greater than 100 mcg/h. Patients may require periodic supplemental doses of a short-acting analgesic for "breakthrough" pain. Some patients may require additional or alternative methods of opioid administration when the DUROGESIC dose exceeds 300 mcg/h.
Pediatrics: DUROGESIC should be administered to only those opioid- tolerant pediatric patients (ages 2 to 16 years) who are already receiving at least 30 mg oral morphine equivalents per day. To convert pediatric patients from oral or parenteral opioids to DUROGESIC, refer to Equianalgesic potency conversion (see Table 2) and Recommended DUROGESIC dosage based upon daily oral morphine dose (see Table 5).
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageDiscontinuation of DUROGESIC: If discontinuation of DUROGESIC is necessary, replacement with other opioids should be gradual, starting at a low dose and increasing slowly. This is because while fentanyl concentrations fall gradually after DUROGESIC is removed, it takes 17 hours or more for the fentanyl serum concentrations to decrease 50%. In general, the discontinuation of opioid analgesia should be gradual in order to prevent withdrawal symptoms.
Opioid withdrawal symptoms (see Adverse Reactions) are possible in some patients after conversion or dose adjustment. Table 3 and Table 4 should not be used to convert from DUROGESIC to other therapies to avoid overestimating the new analgesic dose and potentially causing overdose.